Last week was Brain Health Awareness Week, a timely reminder of how rapidly our understanding of the brain continues to evolve. It also provided the perfect opportunity to revisit some of the most important research developments shaping clinical practice. Looking back at 2025 several key themes stood out not only for their scientific progress, but for their real potential to bridge the gap between research and everyday patient care.
Here are the five topics we think are set to influence brain health and rehabilitation practice in 2026 and beyond!
1. Bimanual Upper Limb Rehabilitation for Stroke
Stroke upper limb recovery research is finally moving beyond basic reach-and-grasp movements to address the complexity of real-world activities. Historically, much of the research has been overly simplified, with improvements demonstrated in functional outcome measures, particularly in higher-functioning stroke survivors, but with limited translation into meaningful real-world activity.
New approaches are now beginning to address this gap. Recent data shows that bimanual performance (using both hands together) improves most significantly within the first six months post-stroke. Importantly, admission grasp function and stroke severity have been identified as the strongest predictors of how well a patient will manage two-handed tasks at one year.
The introduction of clinical decision trees offers a more structured and realistic way for therapists to set goals, helping to better align rehabilitation outcomes with the demands of daily life.
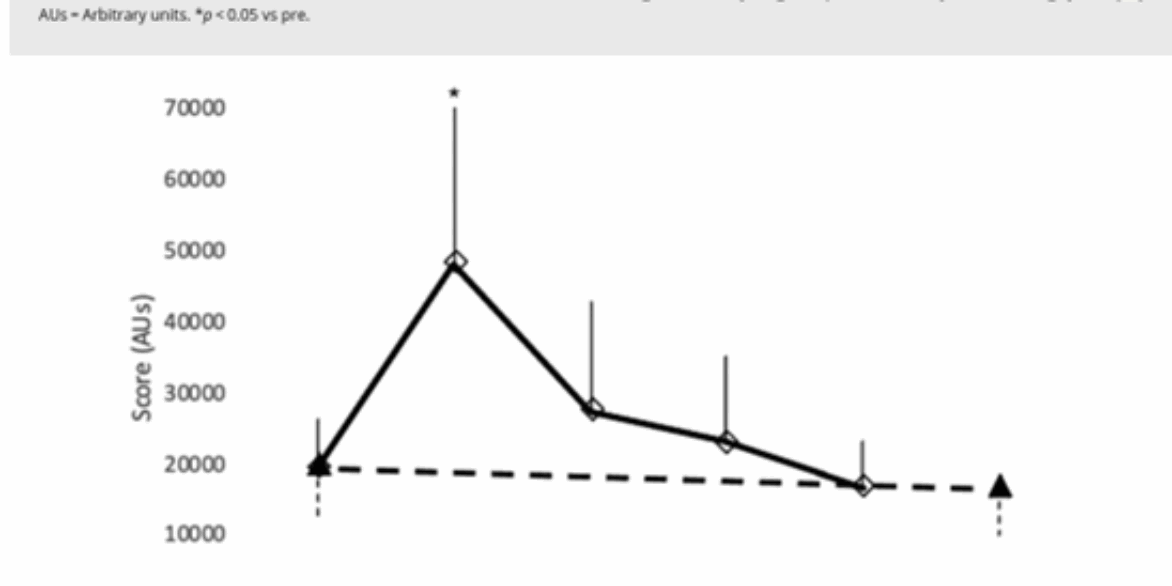
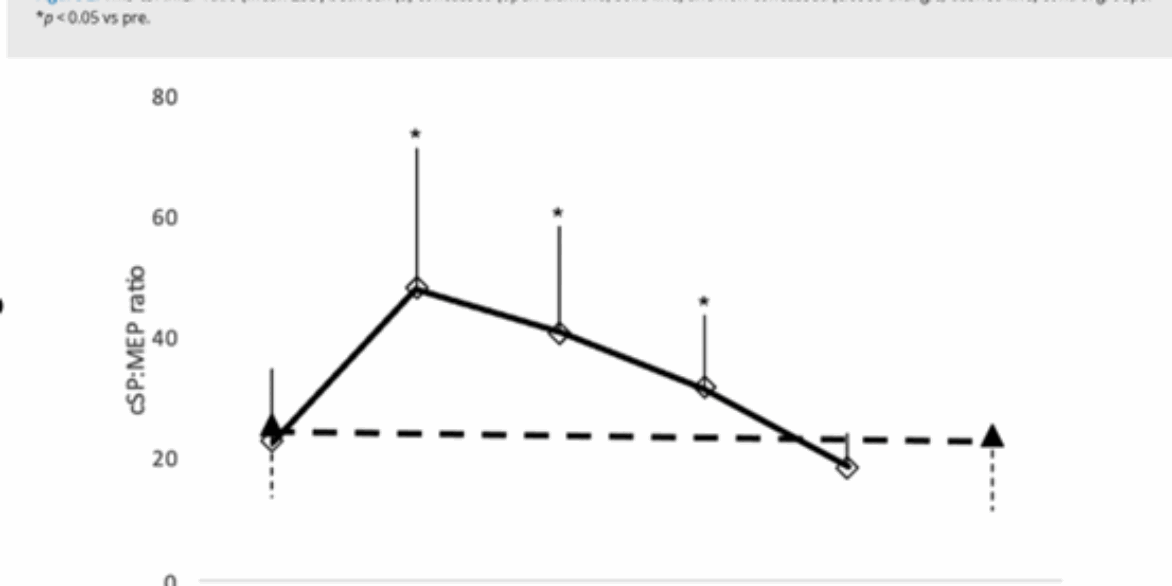
2. Non-Invasive Brain Stimulation (NIBS): Precision and Synergy
After decades of development within research settings, non-invasive brain stimulation (NIBS) is now moving closer to mainstream clinical application, driven by advances in precision targeting and combined treatment approaches.
In Alzheimer’s care, meta-analyses demonstrate that repetitive Transcranial Magnetic Stimulation (rTMS) targeting the dorsolateral prefrontal cortex (DLPFC), alongside transcranial Direct Current Stimulation (tDCS) targeting temporal regions, can significantly improve memory symptoms.
In depression treatment, 2025 saw a notable breakthrough in combination therapy. Using tDCS to “precondition” neuronal activity prior to rTMS has produced response rates of up to 85% within two weeks in treatment-resistant cases.
As understanding of functional brain networks continues to improve, increasingly precise and synergistic applications of these techniques are expected to drive further clinical impact.
3. A Shift in Managing Migraine
The International Headache Society (IHS) has called for a fundamental shift in migraine management; from treating individual attacks to preventing disease progression.
With the emergence of highly effective anti-CGRP therapies, there is now a strong emphasis on early intervention. Treating migraine proactively, before it becomes chronic or high-frequency, offers the potential to reduce both individual burden and wider societal impact, while preserving long-term brain health.
This shift aligns closely with ongoing efforts to improve clinical education and standards across both pharmacological and non-pharmacological management of migraine, supporting a more preventative and holistic approach to care.
4. Exercise for Cognition: The Power of the “Weekend Warrior” and Beyond
With up to 50% of dementia cases now considered preventable, exercise has become a central pillar of brain health and longevity.
New longitudinal research has validated the “weekend warrior” model, showing that individuals who complete their physical activity in one or two sessions per week achieve a 25% reduction in mild dementia risk, outperforming the 11% reduction seen in those who exercise more frequently. This suggests that total volume of activity may be more important than frequency, particularly for individuals with time constraints.
Further strengthening this evidence base, a large umbrella review and meta-meta-analysis published in 2025 confirms that exercise delivers measurable improvements in cognition, memory, and executive function, reinforcing its role as a key intervention in both prevention and treatment.
Key papers:
O’Donovan, G., et al. (2024). Associations of the ‘weekend warrior’ physical activity pattern with mild dementia. British Journal of Sports Medicine.
(2025). Effectiveness of exercise for improving cognition, memory and executive function: a systematic umbrella review and meta-meta-analysis. British Journal of Sports Medicine.
5. Proactive Brain Health Screening for Serious Falls
Proactive brain health surveillance is gaining traction as a practical way to identify risk early and intervene before significant decline occurs.
Simple, measurable markers such as gait speed, grip strength, and mental health indicators are proving to be powerful predictors of outcomes. Research shows that combining gait speed and grip strength can effectively identify individuals at higher risk of serious falls, while monitoring depression and anxiety is increasingly recognised as essential to comprehensive assessment.
A useful way to conceptualise this approach is to think of brain health like a high-performance vehicle. Rather than waiting for a major failure, proactive screening acts as a dashboard of warning lights, allowing early adjustments and maintenance to support long-term performance and resilience.
Digital platforms such as ScreenIT support this multimodal approach, enabling longitudinal health profiling and earlier identification of risk patterns and one of the key reasons why we have developed it.
Several other important research areas narrowly missed this list. As the field continues to evolve, ongoing discussion and collaboration remain essential to translating these developments into meaningful improvements in clinical practice.